






Introduction
Warfarin, as a common oral anticoagulant, is used to prevent and treat thromboembolic diseases such as atrial fibrillation (AF), heart valve replacement, deep venous thrombosis, and pulmonary embolism [1]. Warfarin has many disadvantages such as narrow therapeutic index and wide dose variation of interindividual response, and its stable dosage is influenced by a variety of factors [2]. Thus, determining warfarin therapy is challenging.
Several studies have shown that genetic polymorphisms affect warfarin pharmacodynamics, especially CYP2C9 and vitamin K epoxide reductase complex subunit 1 (VKORC1) [2,3]. One study demonstrated that the VKORC1 genotype can explain about 27% of warfarin dose variation, and the CYP2C9 genotype can explain about 7% of the warfarin dose variation in Asian patients [4]. Combining this with other non-genetic factors, VKORC1 and CYP2C9 in warfarin pharmacokinetics and pharmacodynamics account for approximately 50% of inter-individual warfarin dose variation [5]. However, half of the variation sources are still unknown.
CYP4F2 is an enzyme that can catalyze multiple reactions and affect warfarin dose. CYP4F2 is a primary liver vitamin K1 oxidase that catalyzes the metabolism of vitamin K1 to hydroxy-vitamin K1 and removes vitamin K from the vitamin K cycle, which can lead to less vitamin K available for clotting factor activation [6]. The physiologic role of CYP4F2 in the vitamin K/warfarin pathway is controversial. Some studies have shown that the CYP4F2 genotype can affect warfarin dose. Compared to wild-type patients, patients with CYP4F2 variants need higher warfarin dose [7-10]. But some papers reported that the CYP4F2 genotype did not affect warfarin dose [11-14]. In addition, the CYP4F2 gene influence on warfarin dosage has not been frequently tested in the Korean population. Therefore, we sought to determine if CYP4F2 could affect warfarin dosage in Korean patients with a variety of diseases.
Methods
Study design and patient enrollment
In this observational study, we enrolled 101 Korean patients from the Hospital of Dong-A University between July 2015 and Jan 2018. All patients provided informed consent prior to entering the study. Clinical characteristics, stable warfarin dose, INR, and CYP4F2 genotype were assessed. We collected the clinical data by reviewing electronic and paper medical records, directly inquiring during regularly scheduled clinic visits, and telephone counseling. The clinical data comprised gender, age, height, weight, habits such as smoking and alcohol, target INR, concomitant diseases, combined medications, left ventricular ejection fraction (LVEF), and warfarin stable dosage. The concomitant diseases were AF, thromboembolic disease, heart valve disease, cerebral infarction, coronary heart failure, hypertension, diabetes mellitus (DM), and hyperlipidemia (HLP). The combined medications were β-blocker, amiodarone, angiotensin receptor blocker (ARB), angiotensin-converting enzyme inhibitors (ACEI), aspirin, clopidogrel, statin, calcium channel blocker (CCB), diuretics, and nitrates. We defined body mass index (BMI) as weight (kg) divided by height (m) squared and body surface area (BSA) as {[Height (cm)×Weight (kg)]/3,600}1/2. The stable dose of warfarin was defined as the maintenance dose at which a patient’s INR was within the target range for at least 3 consecutive laboratory measurements separated by at least 1 week [2]. The inclusion criteria were patients who were 20-80 years with body weight above 50 kg treated with warfarin. The exclusion criteria were history of chronic liver failure, treatment with other anticoagulant medication, active malignancy, renal insufficiency (creatinine>2.0 mg/dL or eGFR<45 mL/min), and short life expectancy (<1 year).
Genotyping
Genomic DNA from the patients was isolated from peripheral whole blood using the QIAamp DNA Blood Mini Kit (Qiagen GmbH, Hilden, Germany) according to the protocol of the manufacturer. Genotyping was conducted using SNaPshot assays. The samples were analyzed using an ABI-Prism 3130 genetic analyzer (Applied Biosystems, CA, USA). The SNaPshot results were analyzed by Gene-Mapper® version 3.7 software (Applied Biosystems, CA, USA). The genotype classifications were CYP4F2 GG, CYP4F2 AG, and CYP4F2 AA.
Statistical analysis
Categorical variables were presented as percentage, while continuous variables were presented as mean±standard deviation. For baseline, Pearson’s Chi-square test or Fisher’s Exact Test was performed where appropriate. The correlations between the variables and warfarin stable dose were analyzed by independent samples T test. Oneway ANOVA test was performed for comparing the association between warfarin stable dose and genotype of CYP4F2. Multiple linear regression was performed to model the relationships of dose with other measuring variables and was used to develop a prediction algorithm for warfarin stable dose. In this statistical model, the stepwise selection method was applied to identify significant covariates of the clinical characteristics. Survival data were estimated according to multivariate Cox hazard regression analyses, and the differences between groups were compared with the log-rank test. All statistical analysis was carried out using SPSS software 20.0 (SPSS, Inc., Chicago, IL, USA) with the level of significance set at P<0.05.
Results
Clinical and general characteristics of studied patients
Table 1 summarizes clinical and demographic characteristics of studied patients. The mean age was 64.0±11.9 years. Females comprised 52% of the population. The mean percentage of time in the therapeutic range (TTR) was 52.0±17.3% in the trial. The mean clinical maintenance warfarin dose was 3.26±1.38 (1-9) mg/day. Main indications of treatment were atrial fibrillation (83%), pulmonary thromboembolic disease/deep vein thrombosis (8%), and valvular heart disease and/or valve replacement (9%). Other associated diseases were cerebral infarction (24%), coronary heart failure (31%), hypertension (40%), diabetes mellitus (DM) (20%), and hyperlipidemia (HLP) (8%). One-third of the patients (33%) reported receiving amiodarone. More patients (68, 67%) were treated with diuretics. The patients with higher BMI or higher BSA required significantly higher warfarin dose (P=0.025, P=0.004, respectively). The patients diagnosed with AF had significantly lower warfarin dose (P=0.002). Amiodarone and diuretics significantly reduced warfarin dose requirements (P=0.010, P=0.041, respectively). There were no significant differences for the other clinical characteristics.
Genotype frequency of CYP4F2
For CYP4F2 18000G>A (rs2108622), 46 patients (45.5%) were homozygous for the wild G allele, 44 patients (43.6%) were heterozygous for the wild A allele, and 11 (10.9%) patients were homozygous for the variant A allele. CYP4F2 allele frequencies were 67.3% for the G allele and 32.7% for the A allele (Table 2).
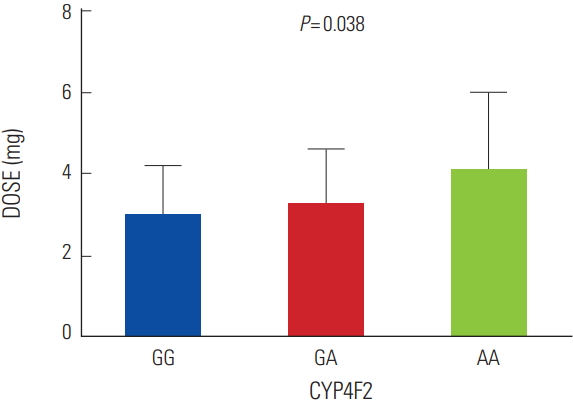
Effect of CYP4F2 18000G>A genotype on warfarin stable dose
As shown in Fig. 1, the mean warfarin dose was higher in patients with the CYP4F2 AA genotype (4.1±1.9 mg per day) compared with that of the GA (3.3±1.3 mg/day) or GG (3.0±1.2 mg/day) genotype. A significant association was observed between warfarin dose and 18000G>A of CYP4F2 (P=0.038).
Clinical factors to determine warfarin dose
From multiple linear regression models, 5 variables were selected as significant factors that influenced the warfarin stable dose: age, BSA, amiodarone, diuretics, and CYP4F2 genotype. The results are presented in Table 3 and Table 4. Sex, smoking, alcohol use, concomitant disease, concurrent medications (except for amiodarone and diuretics), and LVEF were eliminated as predictors because of their weak association with warfarin dose requirements. The predictive contribution of the 5 variables to variability was 33.3% in our model for daily warfarin maintenance dosing.
The equation was: warfarin maintenance dose (mg/day)=4.387+1.053*BSA-0.631*Amiodarone+0.430*CYP4F2-0.335*Diuretics-0.043*Age
The coding was as follows: CYP4F2 18000G>A genotype: input 0 for GG, 1 for AG, and 2 for AA. Amiodarone or diuretics was coded as 1 if present and 0 if absent.
Discussion
CYP4F2 is a vitamin K cycle-related enzyme that metabolizes vitamin K to hydroxyvitamin K. This leads to less vitamin K available for clotting factor activation. The activity of CYP4F2 is reduced in individuals with the CYP4F2 Val433Met SNP (rs2108622, c.1297G>A), resulting in a reduced capacity to metabolize vitamin K and a greater amount of vitamin K to utilize [6]. In addition, CYP4F2 is known to be primarily responsible for metabolizing arachidonic acid to 20-hydroxyeicosatetraenoic acid (20- HETE), which is a potent cerebral artery vasoconstrictor [3]. Many studies have revealed that CYP4F2 gene polymorphisms might be associated with the risk of incident ischemic stroke and myocardial infarction [15,16].
The physiologic role of CYP4F2 in the vitamin K/warfarin pathway is controversial. Most papers posited that CYP4F2 genotype could affect warfarin stable dose to some extent. Julie A et al. illustrated that both Caucasians and Asians required higher warfarin dose with CYP4F2 varients [6]. Caldwell et al. shown that an exonic polymorphism in CYP4F2 was related to the difference of warfarin maintenance dose in a genome-wide association study (GWAS) in Caucasian patients [7]. This paper pointed out higher warfarin dose requirements with the CYP4F2 mutant genotype in Asians [8]. CYP4F2 polymorphism also significantly influenced warfarin dosing variability in the Italian population [9]. In 2010, Cha et al. first established the association of CYP4F2 with warfarin dose in the Japanese [10].
However, some papers showed opposing results. In a total of 207 Egyptian patients, although a trend for dose differences by genotype was observed, there was no significant association between CYP4F2 polymorphism and warfarin dose requirement (P=0.314) [11]. Perini et al. also observed no association between CYP4F2 genotype and warfarin dose requirement in 370 Brazilian patients [12]. In 2011, a Korean group reported that the daily warfarin doses of patients carrying the TT genotype were higher than those of patients carrying the CC genotype (3.5±2.5 vs. 3.0±1.5 mg/day, P=0.0501) [13]. Recently, a study demonstrated that the genotype and alleles of CYP4F2 did not show significant association with the maintenance dose requirements of acenocoumarol in Indian patients with cardiac valve replacement [14]. In our registry, the mean warfarin dose was higher in the patients with the CYP4F2 AA genotype (4.1±1.9 mg/day) compared with that of the AG (3.3±1.3 mg/day) or GG (3.0±1.2 mg/day) genotype. A significant association was observed between warfarin dose and CYP4F2 genotype (P=0.038). We confirmed that CYP4F2 genotype significantly affected warfarin stable dose. In our study, 89.1% patients had either homozygous or heterozygous genotype for CYP4F2 (GG or GA), while 10.9% patients had homozygous genotype (AA), which is similar to a previous study in a Korean population [17].
Our study can explain 33.3% of the variance in warfarin dose based on genetic polymorphisms of CYP4F2 and non-genetic indicators of age, BMI/BSA, amiodarone, and diuretics. Although CYP4F2 genotype mildly influenced warfarin dosage, including this factor in our algorithm can be used to improve prediction of warfarin stable dose.
In several guidelines for the treatment of AF in Western patients [2,18], an INR of PT between 2.0 and 3.0 was recommended for patients with non-valvular atrial fibrillation (NVAF), regardless of age. In contrast, Japanese guidelines recommend a slightly lower INR of 1.6-2.6 for elderly (≥ 70 years) patients [19]. Studies of Asian patients have chosen this guideline as their target INR [20-22]. We also chose this as our target INR.
Limitations
Our study had a limited number of patients, and we only confirmed the influence of CYP4F2 gene on warfarin dose. In our algorithm, we did not include other genetic factors such as VKORC1 or CYP2C9. In the future, we will collect more factors to derive the algorithm to predict warfarin maintenance dose in Korean patients with a variety of diseases.